Can pharmacy-driven medication reconciliation reduce errors and improve patient safety?
When a lack of proper medication reconciliation (MedRec) led to a sharp deterioration in her father’s health Dr Rita Shane (Vice President and Chief Pharmacy Officer at Cedars Sinai Medical Center, Los Angeles, California) promised herself that she would ‘fix’ the problem before she retired. Just 20 years later she succeeded – MedRec by pharmacy staff became a legal requirement in California.
In 1998 Dr Shane’s father underwent a craniotomy for a brain metastasis associated with lung cancer. He developed “intractable agitation” and was transferred to a geriatric-psychiatric unit where his condition became much worse. When Dr Shane asked about his medication it became apparent that the steroids that he had been prescribed after the craniotomy had been abruptly discontinued when he was transferred. “I knew you can’t just ‘cold turkey’ discontinue a steroid in a patient. Ultimately, I had him transferred back to Cedars Sinai because he ended up febrile. He was getting a decubitus [ulcer] and I was concerned that he would die of sepsis in a gero-sych unit due to what I considered an iatrogenic issue”, she says.
Medication reconciliation is often viewed as a simple clerical task. In fact, making an accurate record of current medication is an important procedure because the list becomes the basis for future prescribing decisions. Dr Shane has spearheaded a decades-long campaign to transform this process, arguing that pharmacy staff – pharmacists and technicians – are the only professionals with the specific expertise required to ensure medication safety during transitions of care. This effort recently culminated in California law SB 1254 and subsequent regulatory changes that mandate pharmacy-led MedRec for high-risk patients at both admission and discharge.
The “poly problem” and iatrogenic risk
One important reason for specialised pharmacy intervention is what Dr. Shane calls the “poly problem”: poly-disease, poly-doctor, and poly-pharmacy. As patients over 65 tend to have multiple chronic conditions, they often receive prescriptions from multiple providers and pharmacies. This fragmentation can create a chaotic medication history. In many ambulatory settings, medication histories are entered into the electronic health record (EHR) by medical assistants who, while vital to practice support, may lack in-depth training in pharmacology. These entries then become the “source of truth” for hospital admissions. For example, “When we first implemented our electronic health record, we would see orders like “methotrexate daily” [instead of weekly] that the pharmacist would intercept – and that’s really just a lack of knowledge and skills on the part of people that are transcribing orders without the benefit of the clinical knowledge”, she notes. Dr. Shane compares a medication order to a complex sentence: it requires the correct drug, dose, dosage form, route, rate, and duration. The pharmacist serves as a guardian angel over this process, making sure that orders are complete and accurate in the context of the whole patient, she says.
The evidence: Why pharmacy ownership matters
The push for legislative change was based on rigorous research evidence. Dr. Shane and her team conducted a randomised controlled trial in the emergency department, comparing “usual care” (medication histories taken by busy physicians or nurses) with those taken by trained pharmacy staff. The results were stark: pharmacists and technicians were significantly more accurate, identifying up to eight errors per high-risk patient.
The business case for pharmacy-led MedRec
For healthcare administrators, the argument for pharmacy-led MedRec extends beyond clinical outcomes to financial sustainability. Adverse drug events (ADEs) are a primary driver of increased hospital costs and. Data indicates that an ADE can increase a patient’s length of stay (LOS) – and therefore hospital costs – by an average of 3.1 days. At the time of the evaluation, the cost of a single admission or readmission due to these errors was estimated at $12,000 to $14,000.
By leveraging pharmacy technicians to transcribe histories accurately into the EHR, hospitals can achieve significant savings while allowing nurses and physicians to practice at the highest level of their licenses. One organisation demonstrated savings of $830,000 by utilising technicians for this function. Furthermore, reducing the 40 minutes of nursing time typically spent per patient on medication histories provides a major relief to frontline clinical staff.
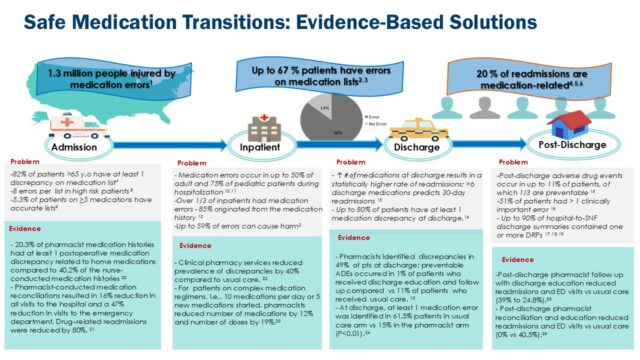
All of this information was brought together in an infographic that was used to educate the State Board of Pharmacy and the California legislature about the problem. “Timing is everything” says Dr Shane and it turned out that one of the California senators was a pharmacist and he enthusiastically supported Dr Shane’s initiative. After a number of hearings, the bill was signed into law in September 2018, just two years and four days after her father’s death. “It was an exciting journey and really an outstanding opportunity to educate legislators”, she recalls. Moreover, during her discussions with legislators, “Everyone seemed to have an example of a family member having a problem with an inaccurate medication list – and that brought it home”, she adds.
Following the passage of SB 1254 (the bill in question) in 2018, a larger study involving 11 California hospitals (ranging from university-based to community hospitals) further validated these findings. Over a six-week period, the study captured approximately 16,000 errors across 2,300 medication histories. Notably, 94% of medication lists contained at least one error, and 25% of those errors were classified as serious or life-threatening. These findings were verified by independent physician reviews, ensuring that the severity of the errors was not overstated. Reflecting on the findings, Dr Shane says, “We demonstrated that we prevented significant harm in the state of California for the hospitals that implemented this new law”.
Closing the loop: MedRec at discharge
While the 2018 legislation focused on admission, Dr. Shane realised that the “back end” of the hospital stay remained a point of extreme vulnerability. She uses the analogy of a totally wrecked car (the patient) that is painstakingly repaired in a body shop (the hospital), only to be driven off a cliff at discharge because the final medication list was inaccurate.
Studies showed that even with accurate admission medication lists, patients still experienced an average of two medication errors at discharge. Approximately 20% of hospital admissions are medication-related, and at least 40% of patients have an error on their discharge medication list, she says. These errors, such as the inadvertent omission of anticoagulants or antibiotics, are then perpetuated by community pharmacists who, lacking access to patient records, have no way of recognising the mistakes.
To address this, Dr. Shane successfully advocated for a regulatory change through the California State Board of Pharmacy’s “sunset review” process. As of January 1, 2026, the law was expanded to include medication reconciliation at discharge for high-risk patients.
A new paradigm: The “high-alert patient”
Perhaps the most transformative concept proposed by Dr. Shane is the shift from focusing solely on high-alert medications to identifying the “high-alert patient”. This designation would apply to the most vulnerable individuals – those with multiple diseases and complex regimens – who should be “tagged” for prioritised pharmacist attention across all providers.
Dr. Shane’s vision is to see these California-led successes become a national standard. Through collaboration with the National Association of Boards of Pharmacy (NABP) and the Joint Commission, she continues to advocate for model legislation that designates pharmacy staff as the clear “owners” of the medication list. For health professionals, the message is clear: ensuring an accurate medication list is not a secondary task; it is a foundational element of patient safety that requires the specialised clinical lens of the pharmacy profession.



