
Putting the findings of the ivermectin meta-analysis into perspective

The Bryant-Lawrie meta-analysis included only randomised controlled trials (RCTs) but evidence from observational trials and real world experience sheds further light on the effectiveness of ivermectin, according to Dr Edmund Fordham, one of the co-authors of the study.
One obvious question is whether the results of the analysis would have been markedly different if observational trials had also been included. Dr Fordham showed how the pooled risk ratio (for infection) was 0.14 (95% confidence interval (CI) 0.90 – 0.21) when RCTs alone were included. This means that the background infection rate is about 296 per thousand in the control group but only about 50 per thousand in the ivermectin group, so 245 per thousand avoid infection. “It is quite a substantial reduction in infection rate”, says Dr Fordham.
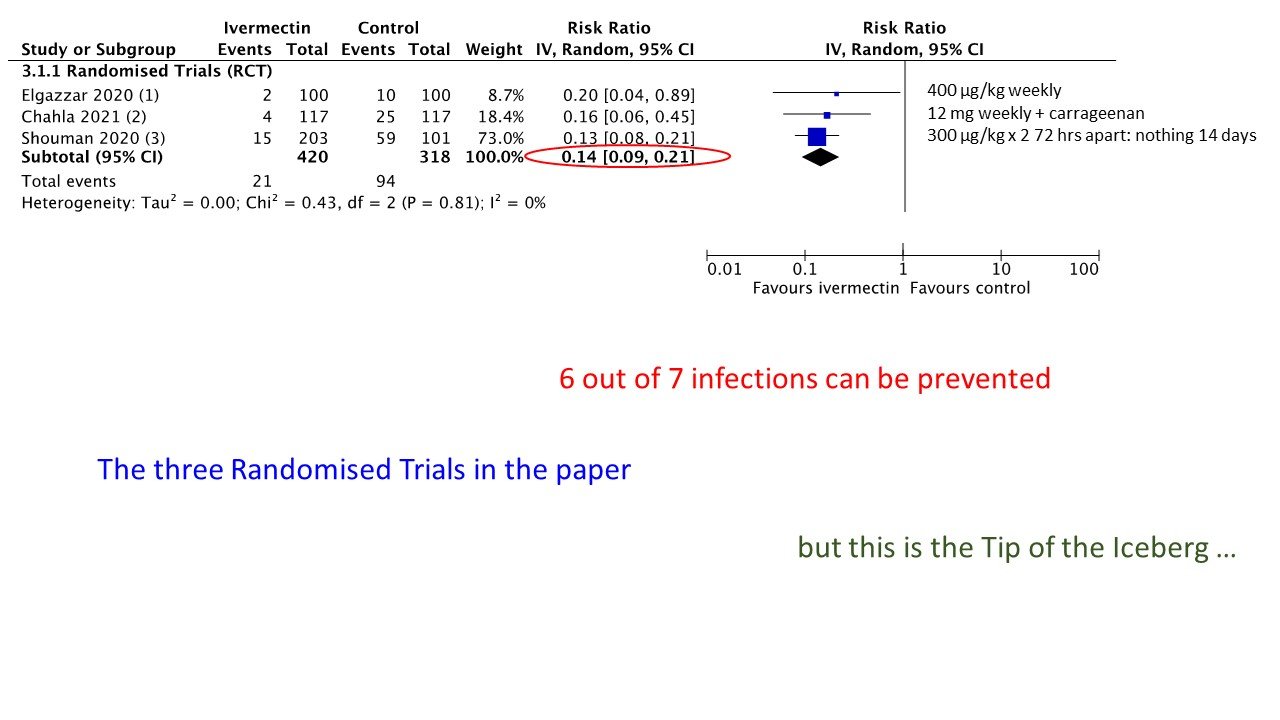
Meta-analysis of RCTs for prophylaxis of covid-19 with ivermectin
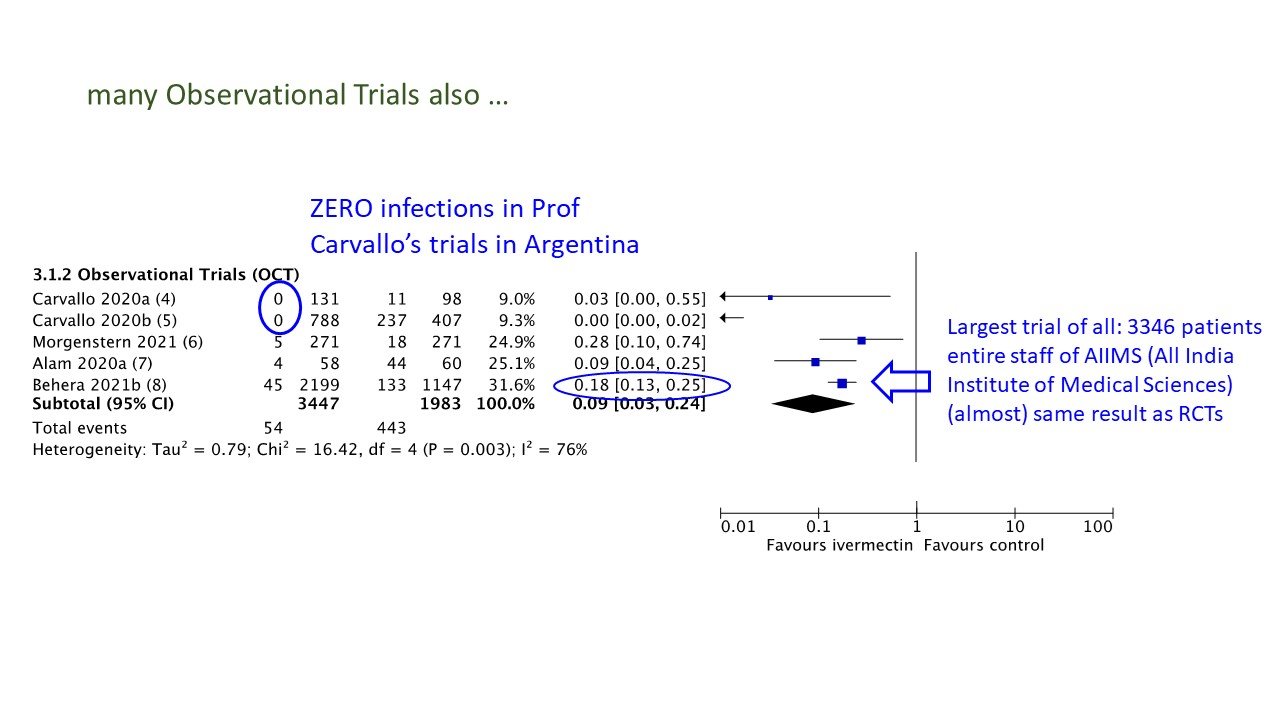
Meta-analysis of observational trials for prophylaxis of covid-19 with ivermectin
Observational trials are considered to provide evidence of lower quality but it is of interest that the observational trials of ivermectin prophylaxis for covid-19 show remarkable consistency. A meta-analysis of observational trials gives a pooled estimate of 0.09 (95% CI 0.03 – 0.24). The studies by Carvallo (Argentina) reported zero infections in the groups that received ivermectin, he noted. The study by Behera (India) was the largest prophylaxis study so far, with nearly 3,500 participants. The result from this study was very similar to the meta-analysis of RCTs with a risk ratio (for infection) of 0.18 (95% CI 0.13 – 0.25).
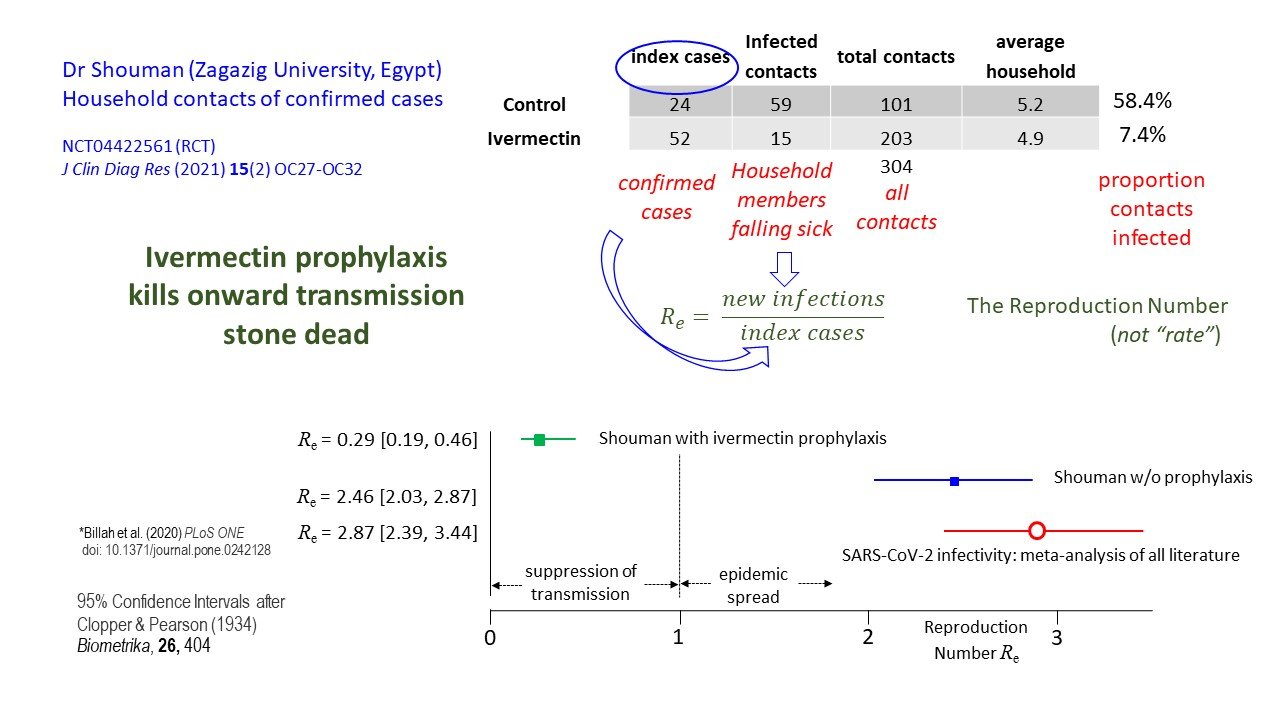
The RCT by Shouman provided additional information. In this trial ivermectin or placebo was given to household contacts of confirmed cases of covid-19 infection.
Ivermectin as potential chemoprophylaxis for covid-19
“Uniquely, amongst all of these prophylaxis trials that I have seen, that enables you to make an estimate of the reproduction number…… the ratio of new infections to index cases” explains Dr Fordham. It follows that the R number with and without ivermectin can be estimated. A meta-analysis of reproductive numbers for SARS-CoV-2 worldwide gave a pooled estimate of 2.87 (95% CI = 2.39 – 3.44). In the study by Shouman, without ivermectin the R number was broadly similar – 2.46 (95% CI = 2.03 – 2.87). However, with ivermectin the R number dropped to 0.29 (95% CI = 0.19 – 0.46). This means that there is very little chance of epidemic spread if household members are all taking ivermectin prophylaxis. “My conclusion is that prophylaxis in the household will kill the onward transmission of the illness stone dead – and I’m really surprised that not more people have noticed this because it really does point to a way of controlling and managing the epidemic ….”, says Dr Fordham.
Mass treatment programmes such as those reported from Peru, India and Mexico also provide evidence of ivermectin’s effectiveness. Dr Fordham emphasises the importance of having a control group to compare the effects of one treatment policy with another.
“In the case of Peru, especially in Mexico and in India you do have those comparisons because some states or regions implemented ivermectin policies and some just refused. And what did we see? Basically the states that refused did much worse than those that adopted the drug”, says Dr Fordham. These experiences are well-summarised on the website of the Frontline Covid-19 Critical Care Alliance, he adds.
Mr Andrew Bryant is a biostatistician and systematic review methodologist based at Newcastle University, in the Population Health Sciences Institute.
Dr Edmund Fordham is a physicist by training with extensive experience in the energy industry (check tape). He is also a long-term non-Hodgkin lymphoma survivor. He works with the Evidence-based Medicine Consultancy as a Consumer Representative.
Read and watch the full series on our website.



